Abstract. To make clinically grounded decisions, medical AI agents are expected to go
beyond simple recognition and be capable of tool retrieval, evidence acquisition, and
integration. Existing benchmarks largely evaluate isolated perception or single-turn
question answering, and therefore provide limited visibility into failures of planning,
tool recruitment, and rollout reliability. We introduce MedCTA, a benchmark for
evaluating medical tool agents on clinician-validated, step-implicit tasks grounded
in realistic multimodal clinical inputs, including radiology images, pathology
slides, and reports. MedCTA comprises 107 real-world clinical tasks with clinician-
verified executable trajectories over 5 deployed tools, and supports process-aware
evaluation of tool selection, argument validity, execution stability, trajectory fidelity,
and outcome quality. We benchmark 18 open- and closed-source multimodal
models and find that even frontier systems remain brittle in multi-step clinical tool
use: autonomous rollouts are dominated by protocol failures, premature stopping,
and incorrect tool recruitment, while gold-standard tool routing yields large but
still incomplete gains. These results show that strong backbone perception does
not translate into reliable agentic behavior in clinical settings. MedCTA provides a
rigorous testbed for auditing, diagnosing, and advancing trustworthy medical AI
agents.
Clinical decision making is iterative and multimodal: agents must inspect images, extract text, measure
findings, retrieve knowledge, combine evidence, and stop only after the conclusion is supported. MedCTA
turns that requirement into an executable benchmark where the tool sequence is hidden from the model and
must be planned autonomously.
Task tuple
Each task is represented as (X, Q, U, π, A): clinical context, step-implicit
query, hidden sufficient tool subset, reference interaction trace, and final clinical outcome.
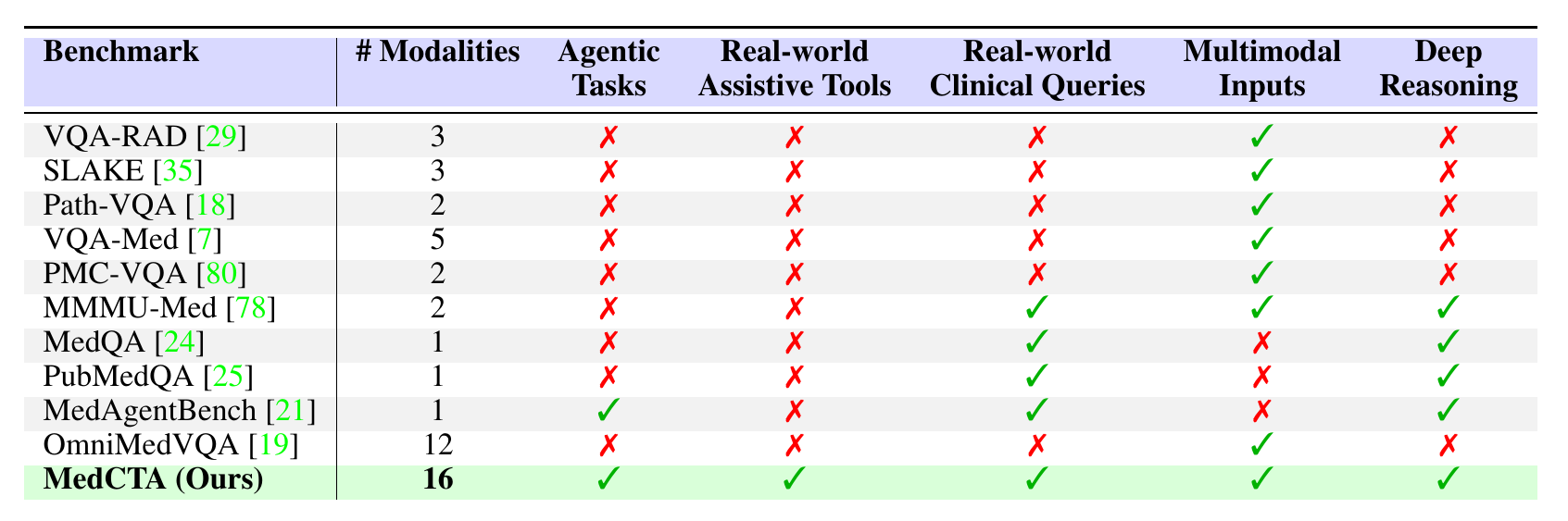
Table 1. MedCTA is positioned against representative
medical VQA, medical reasoning, and medical agent benchmarks, emphasizing executable tools,
real-world clinical queries, multimodal inputs, and deep reasoning.
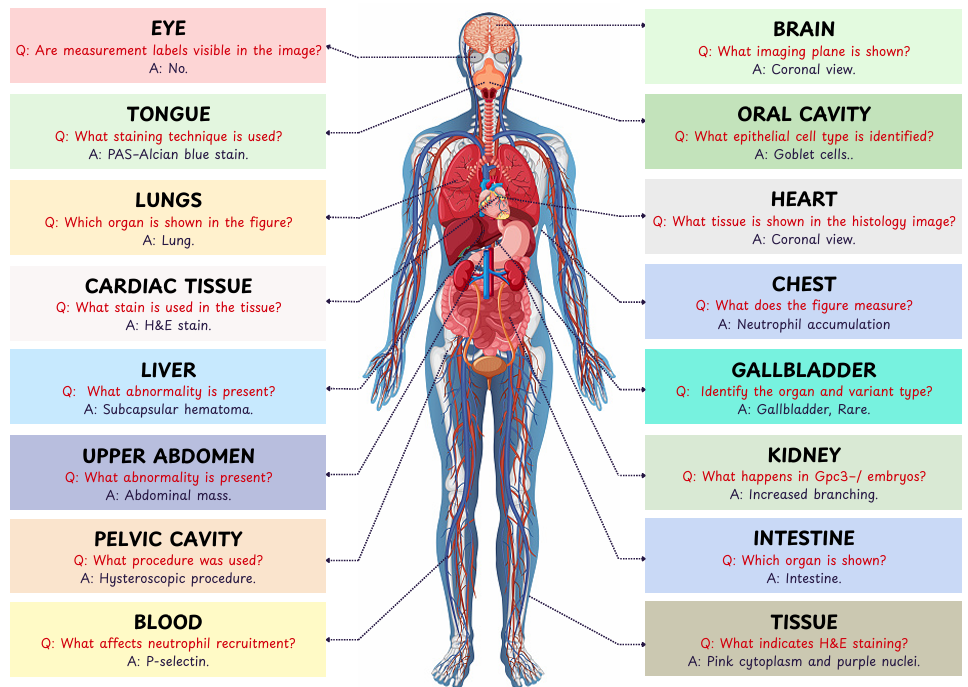
Clinically Grounded, Tool-Implicit Tasks
MedCTA starts from perception-level medical QA seeds and lifts them into realistic clinical objectives.
LMM drafts provide scalable starting points, human annotators remove tool leakage and procedural
phrasing, and clinicians verify medical correctness, workflow plausibility, and final outcomes.
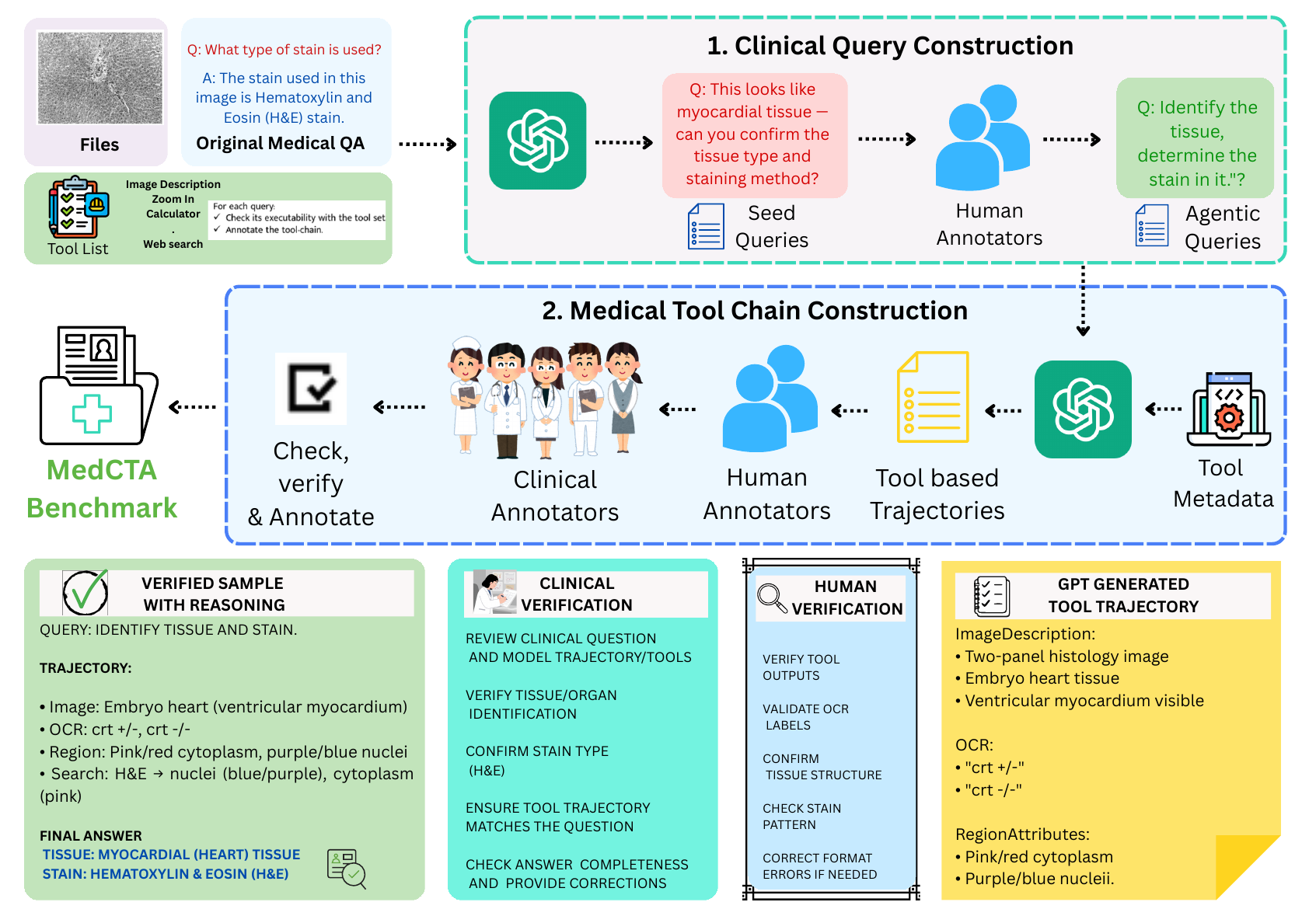
Figure 1. MedCTA construction combines clinical query construction with
medical tool-chain construction. Technical and clinical reviewers ensure executability,
minimality, and medical soundness.
Clinical query construction
Final queries are goal-oriented and clinically phrased. They require multi-step tool use but do
not reveal which tools should be called or in what order.
Reference trajectory construction
Candidate trajectories are drafted by an LMM, technically refined for schema compliance and
minimality, then clinically verified for evidence grounding and reasoning soundness.
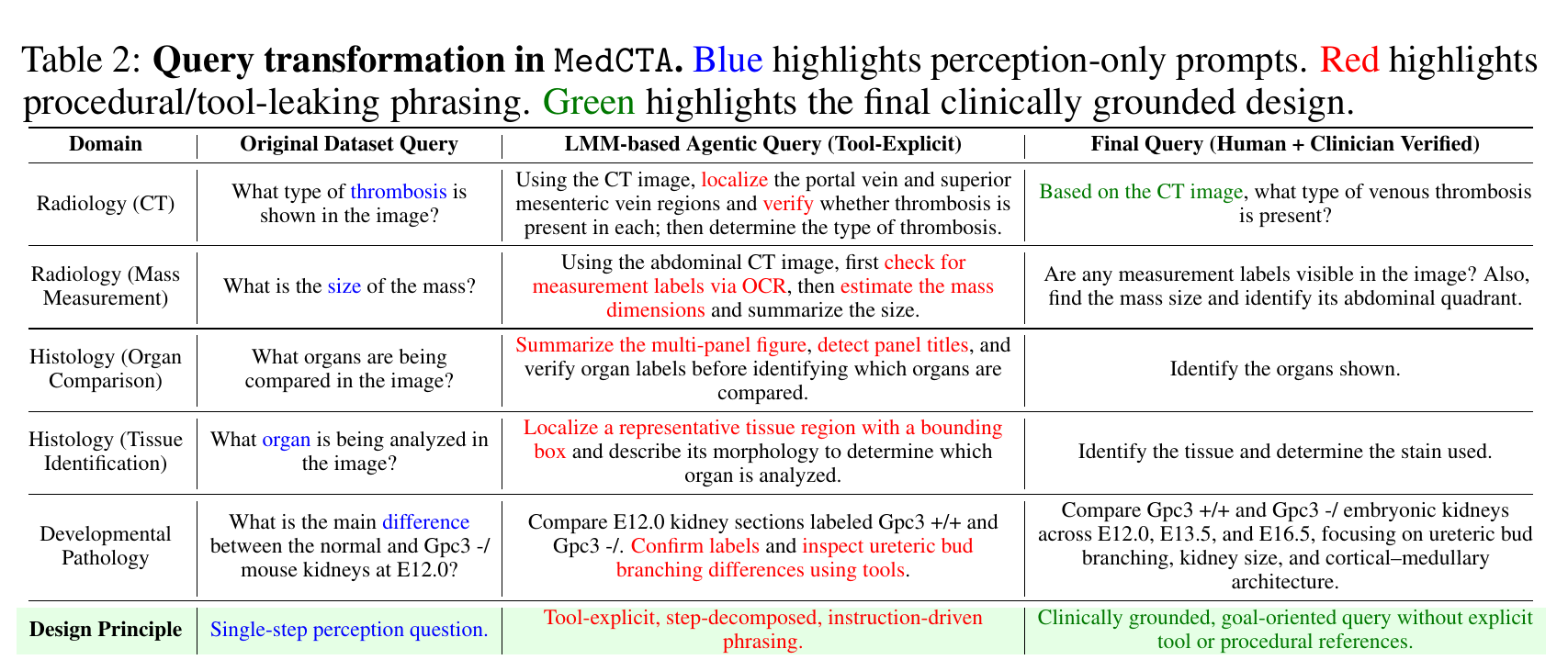
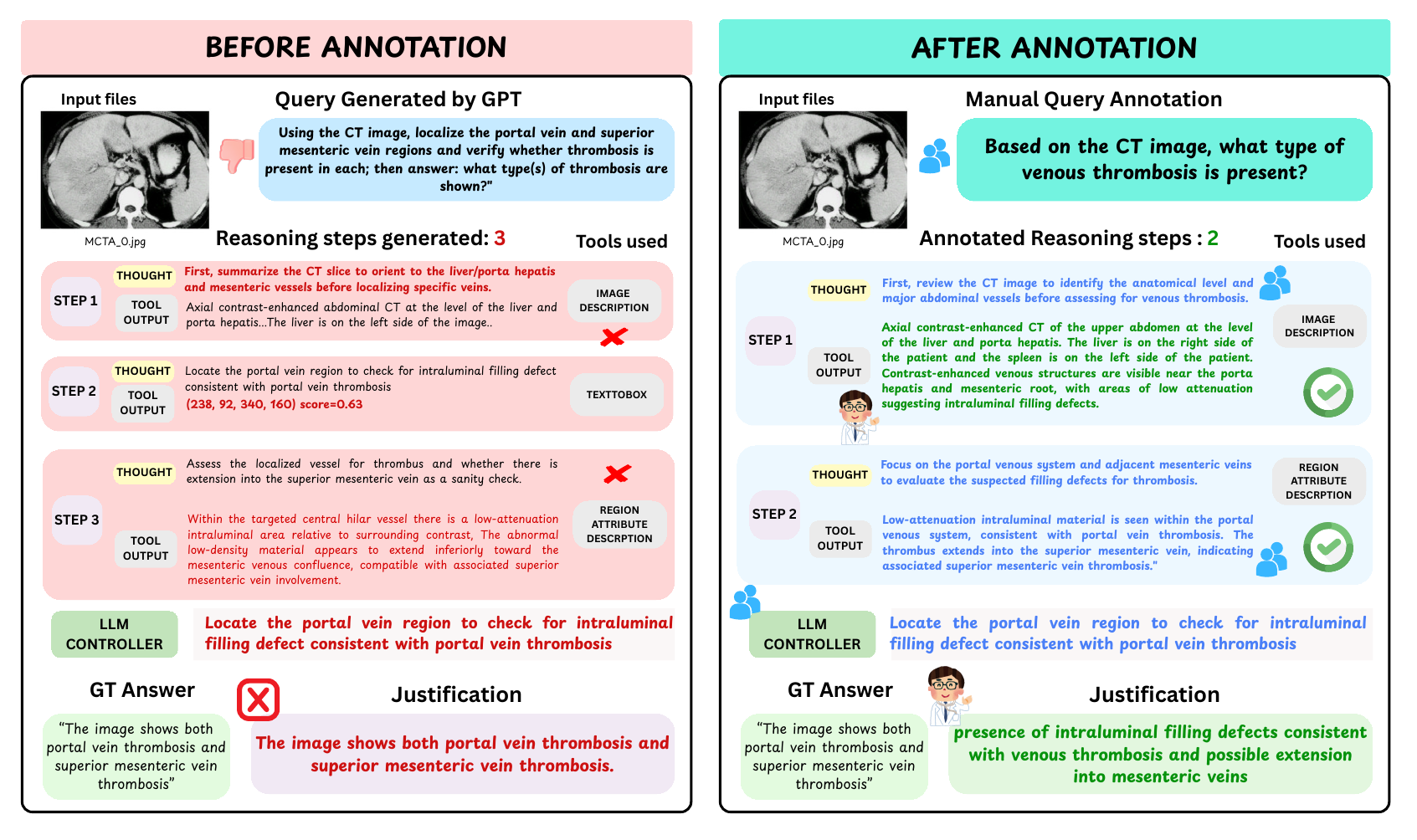
Table 2. Query transformation removes perception-only prompts and
tool-leaking instructions, leaving a clinically grounded goal that still requires planning.
Figure 2. Human and clinician review shortens brittle LMM-generated
trajectories while preserving the medical evidence needed to answer the query.
Broad Multimodal Clinical Coverage
321human annotation
hours
34anatomical regions and
body systems
2-4tool steps per
task
3.1average
tool-execution steps
Executable tool library
Tool
Purpose
OCR
Extract visible text from images and documents.
ImageDescription
Generate holistic visual summaries.
RegionAttributeDescription
Describe attributes in localized image regions.
GoogleSearch
Retrieve external knowledge for a query.
Calculator
Evaluate symbolic and numerical expressions.
Modality coverage
The benchmark mixes radiology, pathology, report-based inputs, microscopy, fundus photography,
and other clinical image types.
CT
20.0%
Reports
20.0%
Histopathology
18.3%
X-ray
9.6%
MRI
8.7%
Fundus
7.0%
Trajectory-Aware Evaluation
MedCTA reports three complementary metric groups: step-by-step tool-use fidelity, clinical reasoning
quality, and final outcome accuracy. This makes it possible to identify whether a model failed because
it chose the wrong tool, produced invalid arguments, drifted away from evidence, or reached the wrong
clinical conclusion.
Metric group
Metrics
What it diagnoses
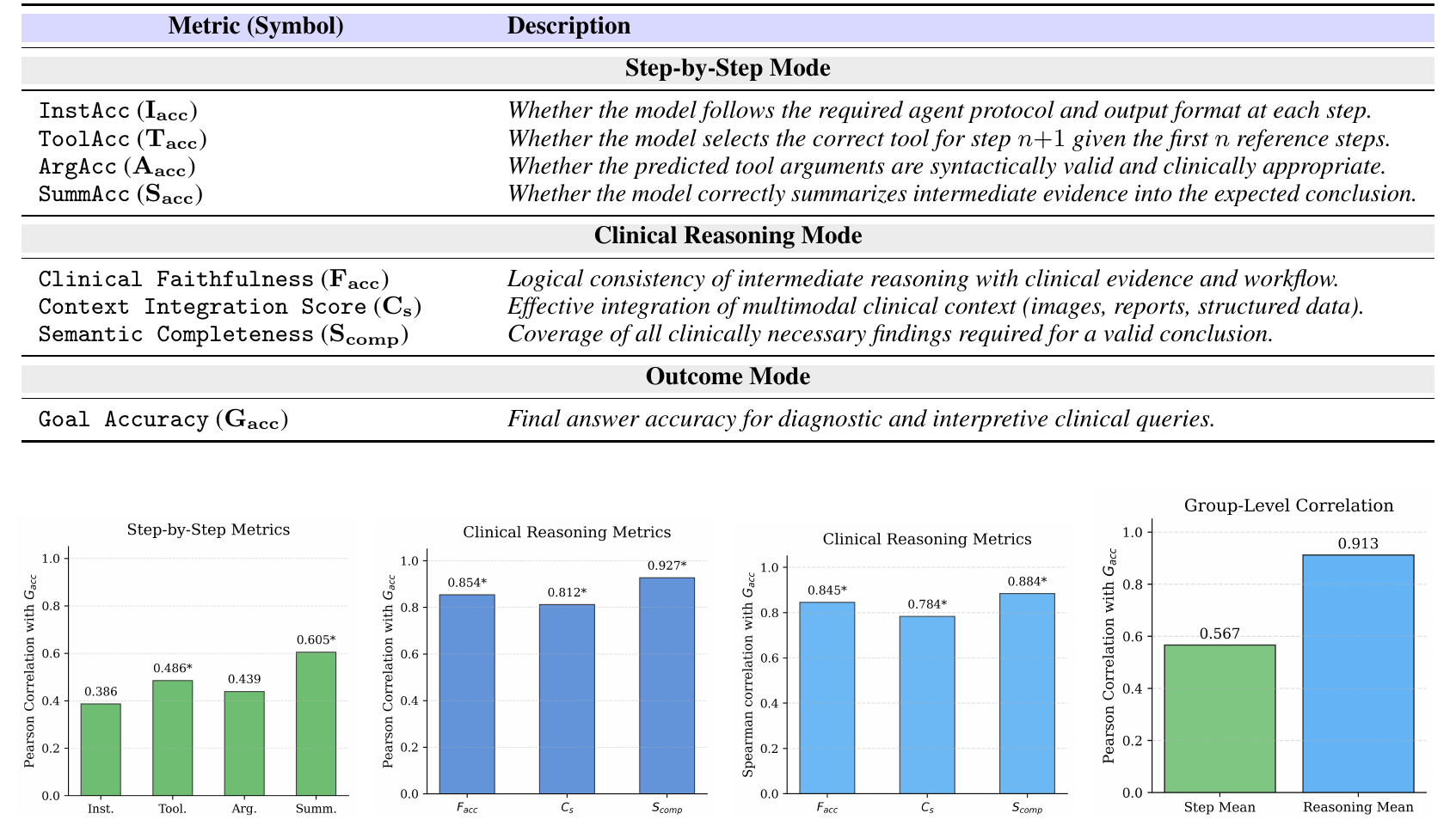
Step-by-step
InstAcc, ToolAcc, ArgAcc, SummAcc
Protocol adherence, next-tool selection, argument validity, and intermediate
summarization.
Clinical reasoning
Facc, Cs, Scomp
Clinical faithfulness, multimodal context integration, and semantic completeness.
Outcome
Gacc
Final answer accuracy for diagnostic and interpretive tasks.
Table 3 and Figure 3. Clinical reasoning metrics, especially semantic
completeness and clinical faithfulness, correlate strongly with final accuracy.
MedCTA Leaderboard
In the autonomous tool-using setting, the best reported outcome accuracy is 31.54%. The
strongest open model reaches 27.80%, while gold-standard tool routing produces large
gains, indicating a major controller reliability gap.
Model
Family
Step-by-Step
Clinical Reasoning
Gacc
Inst.
Tool.
Arg.
Summ.
Facc
Cs
Scomp
GPT-5.4* closed
OpenAI
35.27
23.46
12.61
35.51
17.52
14.21
18.60
31.54
GPT-5.4-mini* closed
OpenAI
5.36
6.74
3.23
0.93
16.47
10.56
17.29
28.31
GPT-5.4-nano* closed
OpenAI
33.93
18.18
12.02
34.24
18.43
11.96
14.77
20.30
GPT-oss-20B open
OpenAI
1.79
0.00
0.00
0.00
1.31
0.56
1.68
3.18
Claude-opus-4-6* closed
Anthropic
24.78
8.80
0.59
39.25
14.11
14.86
23.83
31.32
Claude-sonnet-4-6* closed
Anthropic
23.66
4.99
0.00
33.64
12.77
12.90
20.19
25.33
Claude-haiku-4-5* closed
Anthropic
27.46
13.78
4.69
43.93
9.35
3.36
14.11
23.08
Gemini-3-flash* closed
Google
3.35
17.30
0.00
5.61
11.31
8.60
15.98
25.87
Gemini-3-flash-lite* closed
Google
2.90
8.21
0.00
1.87
10.75
6.82
14.58
23.64
Qwen3.5-9B open
Qwen
44.20
14.37
13.78
29.91
10.37
17.10
13.36
21.64
Qwen3-8B open
Qwen
33.93
10.56
7.04
32.71
8.50
10.09
11.50
27.80
DeepSeek-R1-Distill-7B open
DeepSeek
10.49
3.52
0.00
7.48
2.62
0.84
3.36
10.61
Deepseek-llm-7b-chat open
DeepSeek
11.61
6.45
0.00
4.67
4.30
2.62
4.02
11.00
DeepSeek-V2-Lite-Chat open
DeepSeek
11.83
11.14
0.29
0.00
3.83
3.55
6.54
6.96
Llama-3.1-8B-Instruct open
Meta
23.66
7.92
0.00
6.54
7.94
5.42
11.21
18.94
Llama-3.2-3B-Instruct open
Meta
18.53
1.76
0.00
4.67
3.08
1.68
5.14
11.29
Mistral-7B open
Mistral
18.75
14.66
0.00
9.35
2.52
1.87
3.46
9.40
Phi-4 open
Microsoft
20.09
6.45
0.00
14.02
6.36
3.36
6.17
10.65
Controller Failures Dominate Rollouts
Gold-routing gap Claude-opus-4-6 improves from 31.32 to 66.40 Gacc
when tool routing is provided.
Under-calling 99.2% under-call rate indicates premature stopping
before sufficient evidence is collected.
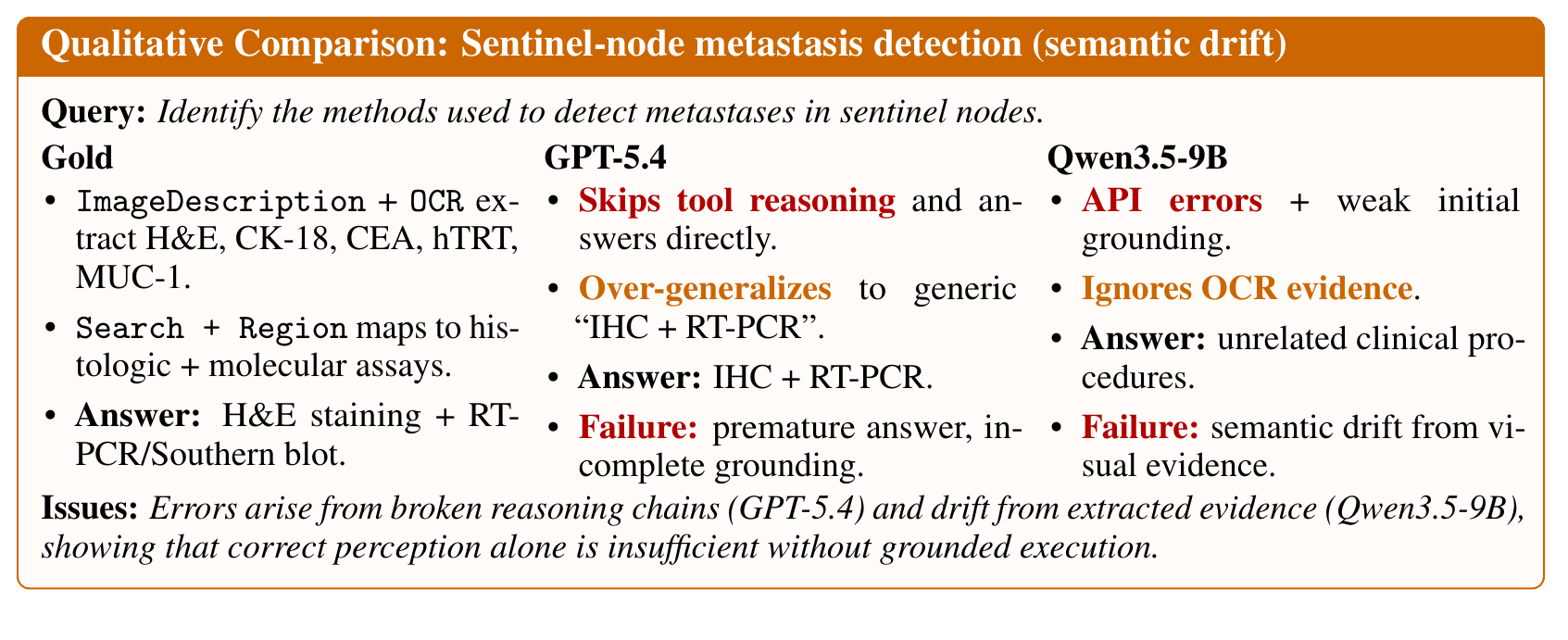
Figure 4. A sentinel-node metastasis example shows how models can skip
tool reasoning or drift away from extracted OCR evidence, even when perception is recoverable.
Reliable Clinical Agency Requires More Than Perception
MedCTA shows a separation between backbone perception and agentic competence. Strong VLMs can identify
medical content in a single turn, but autonomous clinical tool agents must also select tools, maintain
valid interaction protocols, integrate intermediate evidence, and stop only when the answer is
justified.
Backbone-only comparison
Several backbone VLMs score higher without tool interaction than many autonomous tool-agent
rollouts, which indicates that agent control is itself a major research problem.
What to improve next
Future clinical agents need stronger tool recruitment, stable protocol execution, stop/continue
calibration, and evidence-obedient reasoning over localized multimodal observations.
BibTeX
@misc{medcta,
title={MedCTA: A Benchmark for Clinical Tool Agents},
author={Tajamul Ashraf and Hyewon Jeong and Fida Mohammad Thoker and Bernard Ghanem},
year={2026},
eprint={2606.11702},
archivePrefix={arXiv},
primaryClass={cs.CV},
url={https://arxiv.org/abs/2606.11702},
}